
The Language of Value in Healthcare
The Language of Value in Healthcare
Or 'why don't people care about how many users I've got?'


tl;dr-
One major barrier to healthcare evolution globally is the lack of consensus on how to measure ‘value’ for healthcare products, services, & business models
This lack of consensus reduces the ability for different stakeholders to collaborate effectively with one another; one stakeholder may perceive a specific asset as valuable & promote its adoption, while another may not & begin implementing barriers to adoption
One easy example of this heterogeneity is patient value vs. payer value; while patients define ‘value’ in terms of efficacy, convenience, and patient OOP on an individual level, payers define ‘value’ in terms of decrease in budget impact, decrease in resource utilization, and efficacy on a population level
Another much more stark example - one facing many digital-forward innovators - is for digital health companies vs. payers. While digital health companies use engagement as a proxy for value (i.e. ‘the more a patient uses + the more patients using an intervention, the more valuable it must be’), engagement metrics do not substitute in payer minds for efficacy measures on a population level (i.e. improving a clinical endpoint)
Accordingly, moving healthcare forward will require a couple of prerequisite conditions:
A common definition of value for healthcare products, services, & business models across all stakeholders
Processes that align stakeholders around that definition to support & promote collaborative decision-making between industry stakeholders
Consideration of these measures in product design & development processes, whether it is a new drug, medical device, or digital health product
* * *
I’m sure some of you reading this are screaming interally, ‘but there IS already a definition of value for healthcare; it’s quality divided by costs!'1 or ‘but there IS already a common measure of value for healthcare; it’s the Quality-Adjusted Life Year (QALY)!’2 While there is value in these concepts as foundational frameworks - the former, an effective ‘easy to understand’ mnemonic that centers individuals, the latter being the ‘alpha version’ of how to measure value dating from the 1970s3 - our understanding of the deep interconnectivity between health, society, and overall consumer behavior & experience has created a need for more sophisticated measures. In particular, QALYs - and organizations that assess products based on this methodology, such as ICER4 - have long been criticized not only with how specific outcomes are incorporated into the model, but also what outcomes are left out of the methodology entirely.5 This has resulted in vigorous debate across the industry6, as well as a rather tepid adoption of QALY methodology7 in the absence of government support.8
The point of the above paragraph, however, is not to make the case that QALY is good or bad - but to showcase how much dissention there is across the industry on what truly is the appropriate measure of value.9 This issue - a people & process problem, as opposed to a technology problem - breaks the ability for different stakeholders to collaborate with one another on different initiatives in healthcare. For example, the highly popular concept of value-based care (VBC)10 completely falls apart if HCP & payer stakeholders cannot agree on a common definition of value. Even if there is a common goal to strive for, it is unreasonable to expect stakeholders to work together if each measures progress towards that goal in a different way & measures the value of achieving that goal differently. After all, even if you and I both agree to dinner - but I value taste, you value cost, and we don’t move to compromise, we’re just not going to go to dinner.
One of the ways the industry is reacting to this is, well, side-stepping it completely. Consider the following graphic:
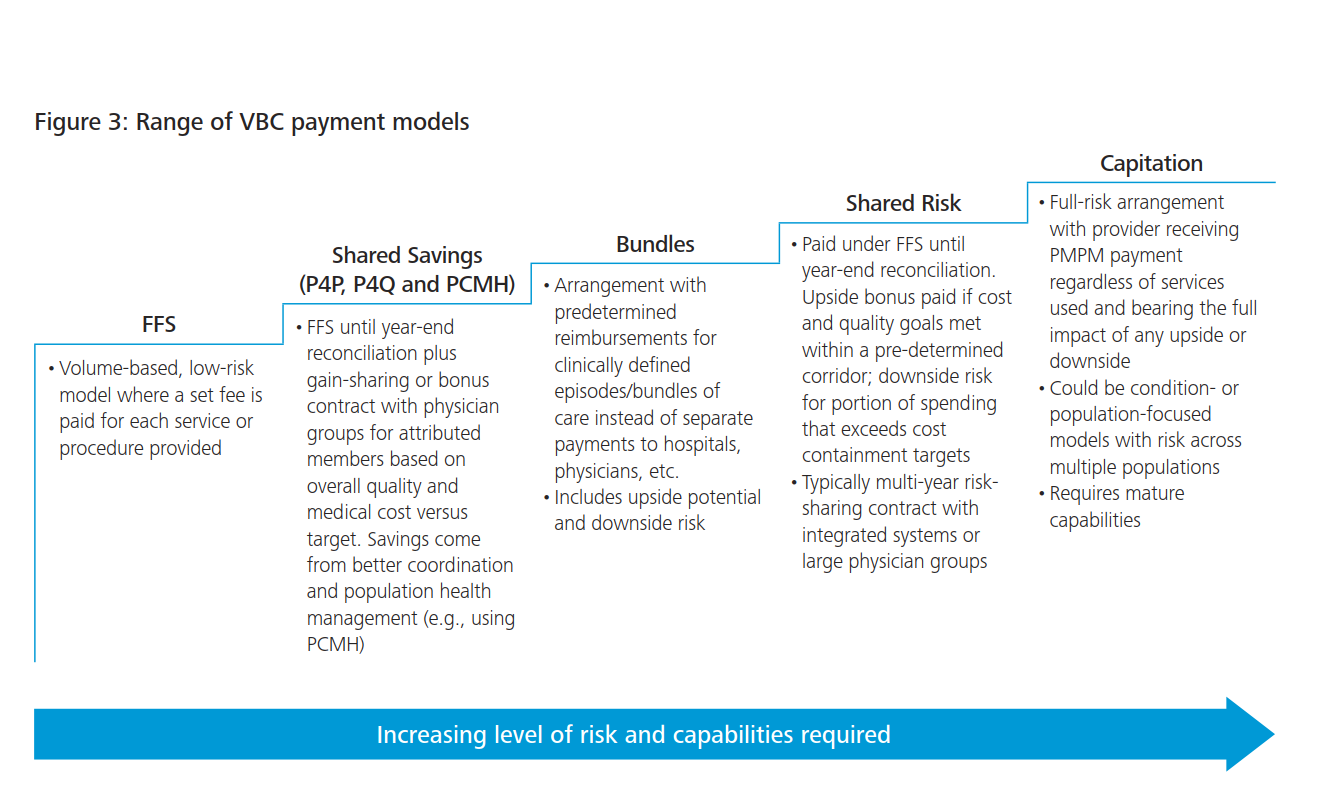
Without getting into details, what should be the most striking about this (very excellently crafted) resource is how the approach to aligning definitions of value is simply telling the payer to not worry about it, facilitated by the HCP taking increasingly larger amounts of risk (up to, of course, full capitation). This system is far less about collaboration between provider & payer, and more on sidestepping the potentially awkward conversation of value altogether in favor of a ‘don’t worry, we got this - just pay us’ attitude. It’s a little amusing because it seems to paradoxically go against one of the major trends in healthcare today - the increasingly widespread fusion of payer & provider entities.
One other way the industry is reacting is to try and create better measures - whether that is improving on existing ideas, or trying new methodologies altogether. This isn’t necessarily just finding alternatives to the QALY (though certainly, people are trying11), but stems from turning the problem on it’s head - ‘why do we need to align on a definition of value, if we can just measure everything?’ When viewed from this perspective, there is a large amount of interplay because the creation of better measures & their operationalization12, centered around - to the surprise of no one - real world evidence (RWE)13. One major open question is in a world with full data transparency between clinical outcomes & cost, is there even a need for a framework measure like the QALY vs. just directly measuring how much value each use of an intervention represents? Perhaps we have all been asking the wrong question - it’s not about the definition of value, but how we may prepare for a world in which no matter how we may choose to define it, we can instantly assess value immediately either at point of care, or point of sale.
But to pull you back to earth - and away from a future world of instantaneous value assessment & everyone knowing exactly how good a product is & how much it should cost, success in healthcare for the foreseeable future will rely on navigating different definitions of value - and knowing what evidence to generate to determine a product’s performance in each one. This seems to be a hard lesson to innovators moving into healthcare from the technology side, as my subtitle cheekily alludes to. After all, value in consumer tech is often measured in terms of engagement - how many users, how often do they spend on your tech, how durable is their utility, etc.14 - but not oftentimes on the actual ‘benefit’ that tech has had on a person’s life (for example, how ‘happy’ they may be15). In healthcare, however, the benefit and how you measure it is king - a 1+1=2 fundamental - so it should come as no surprise that innovators used to thinking about value simply as community-building, Monthly Active Users (MAUs), or number of downloads face an abrupt shock moving into healthcare. At least we’re finally seeing some nice resources from digital health thought leaders addressing this divide.16
I’ll end my thoughts here with a repeat of a refrain I’ve been echoing for a while now. Sing it with me!
There is, at least for right now, no real B2C-only model in healthcare because of the lack of individual buying power (for various macroeconomic reasons).
The major path to sustainability (outside of owning infrastructure) is reimbursement either by a payer or an employer.
That reimbursement is conditioned on certainty that the payer is paying for something that works.
Critical to that is understanding how value is measured - and how your solution can generate evidence that proves that value.
A final aside. While navigating all these dynamics may seem complex, one thing (at least to me) is very certain. You may be able to get that high valuation or a pump piece from a VC firm in the short term off of hype & a great story, but it won’t get you to the finish line you’ve promised yourself, your employees, or the patients you’re serving17 without evidence that your big idea actually works.
https://www.ncmedicaljournal.com/content/77/4/276
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC317370/
https://scholarship.law.duke.edu/cgi/viewcontent.cgi?referer=https://en.wikipedia.org/&httpsredir=1&article=3493&context=lcp
https://icer.org/
https://www.fightchronicdisease.org/latest-news/health-care-valuations-based-qaly-undercut-fight-against-chronic-disease
https://www.nmqf.org/nmqf-media/traditional-value-assessment-methods
https://www.healthaffairs.org/do/10.1377/hp20210823.886249/full/
https://www.statnews.com/2019/02/22/qaly-drug-effectiveness-reviews/
https://ncd.gov/sites/default/files/NCD_Quality_Adjusted_Life_Report_508.pdf
https://link.springer.com/article/10.1007/s10728-019-00381-x
https://pubmed.ncbi.nlm.nih.gov/27139424/
https://www.managedhealthcareexecutive.com/view/top-5-barriers-value-based-care
https://pubmed.ncbi.nlm.nih.gov/9069609/
https://www.ispor.org/docs/default-source/presentations/91154pdf.pdf?sfvrsn=ba921ec5_0
https://www.mckinsey.com/industries/life-sciences/our-insights/real-world-evidence-from-activity-to-impact-in-healthcare-decision-making
https://www.sitecore.com/knowledge-center/getting-started/what-is-engagement-value-and-how-to-use-it
https://www.forbes.com/sites/tomokoyokoi/2021/03/27/pursuing-happiness-in-a-digital-world/?sh=4425afb14471
https://a16z.com/2021/10/19/the-new-go-to-market-playbooks-for-digital-health-startups/



